If you're interested in orthopedics you'll definitely want to check this review out!

The ankle is a complex hinge joint comprised of the tibial plafond, talar dome, and distal fibula.
Ankle fractures most commonly occur in elderly females, with roughly 70% being isolated malleolar, 20% being bimalleolar, and 5-10% being trimalleolar. (1)
When first examining a patient with an ankle injury, you can utilize the Ottawa Ankle Rules to determine if you should x-ray the patient.
Our review of The Ottawa Ankle Rules can be found here:
https://x.com/Ortho_Reviews/status/1278704611218665472
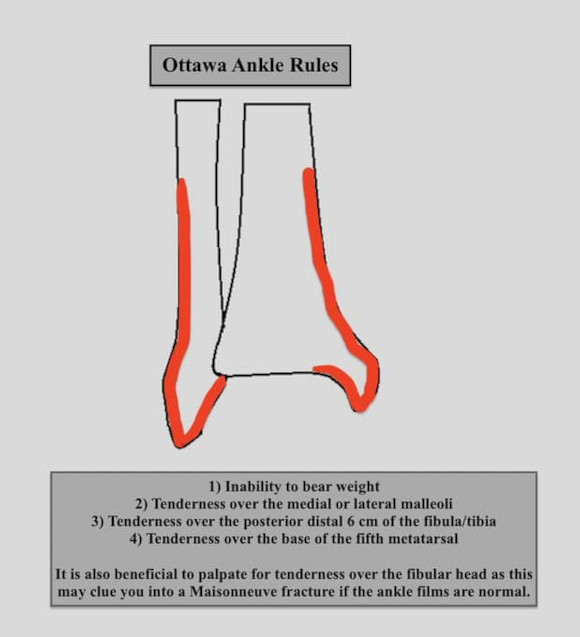
A Maisonneuve fracture is a spiral proximal fibula fracture, that should be suspected in a patient with tenderness over the fibular head after an ankle injury.
Ankle radiographs may be normal and if not vigilant this fracture may initially be missed.

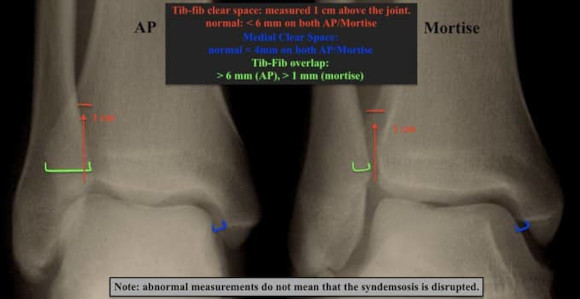
There are three views in an ankle series: AP, Lateral, and Mortise. A mortise view is taken with the ankle in 20° internal rotation.
The syndesmosis can be assessed radiographically by an ER stress view, gravity stress view, or by using measurements on AP/mortise views.

Normal radiographic measurements suggesting syndesmotic stability:
Medial Clear Space:
✯ < 4 mm on AP/mortise
Tib-fib Clear Space:
✯ < 6 mm on AP/Mortise
Tib-fib overlap:
✯ > 6 mm on AP
✯ > 1 mm on Mortise
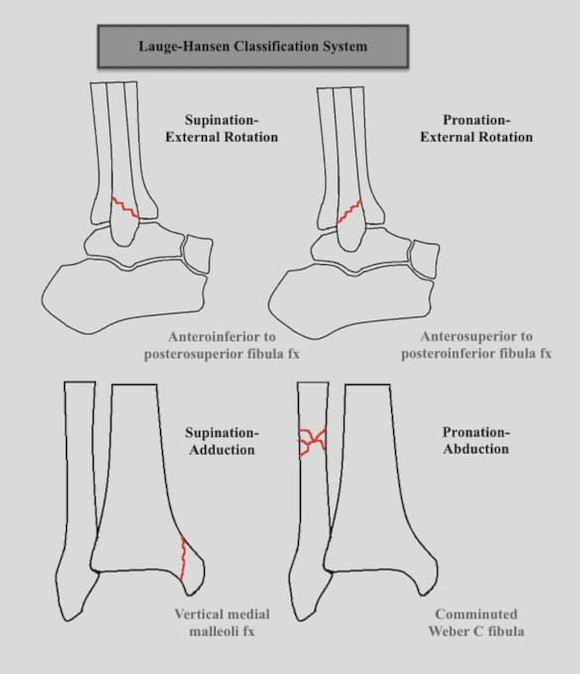
There are two main classification systems for ankle fractures. Lauge-Hansen and Webers.
Lauge-Hansen describes ankle injuries as the position of the foot and then the force applied.
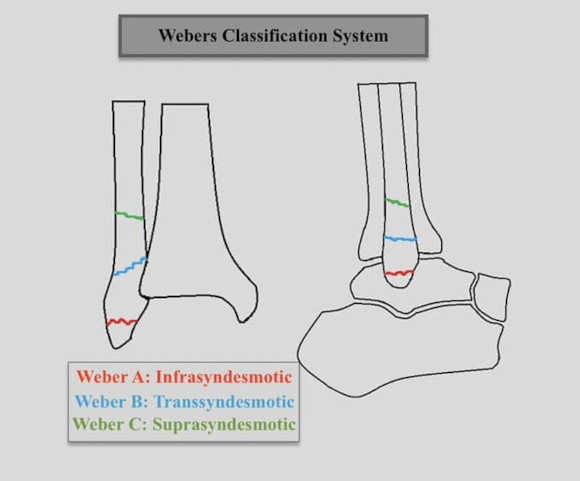
Weber classifies fibula fractures based on their relation to the syndesmosis.
The Lauge-Hansen system has 4 types and each has a unique feature (shown below). Lauge-Hansen stages these fracture patterns from stages 1-4 and it is much more detailed than presented here. This is an extremely simplified version but knowing the unique features will allow you to quickly determine which type of ankle fracture you’re viewing.
Webers classification system classifies distal fibula fractures based on their orientation to the syndesmosis.
Weber A: infrasyndesmotic
Weber B: transsyndesmotic
Weber C: suprasyndesmotic
The more proximal the fracture the higher likely hood of syndesmotic disruption.
Another eponym fracture to be aware of is the Bosworth fracture (shown below). This occurs when the proximal fibular fragment becomes fixed on the posterior tibial tubercle.
This type of fracture pattern can hinder reduction.

Another type of ankle fracture to be aware of is the bimalleolar equivalent. This fracture occurs when there is an isolated lateral malleoli fracture with disruption of the syndesmosis. (shown below)

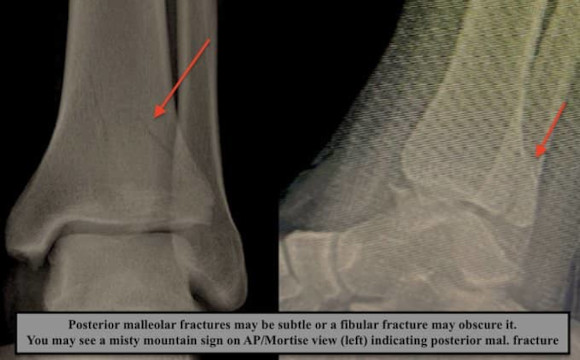
Posterior malleolar fragments may be subtle or obscured by a fibular fracture.
You may see a misty mountain sign (left) or a double contour sign indicating a posterior malleolar fracture.
Operative Indications:
Bi and tri-malleolar fractures.
Bi-malleolar equivalents.
Bosworth fractures.
Open fractures.
Posterior malleolar fragments with >2 mm articular step-off or >25% joint involvement.
Fractures are treated with ORIF and treatment depends on the fracture pattern.
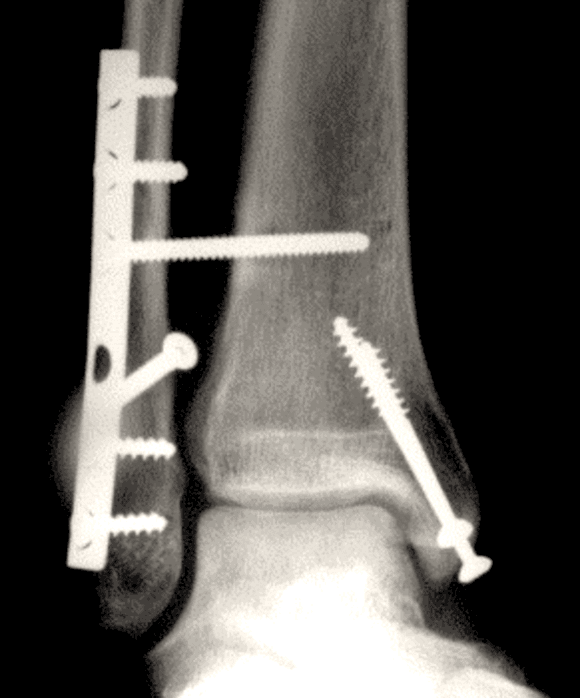
Lateral malleolar fractures may be treated with a lag screw + neutralization plate, fibular nail, or anti-glide plate (shown below).

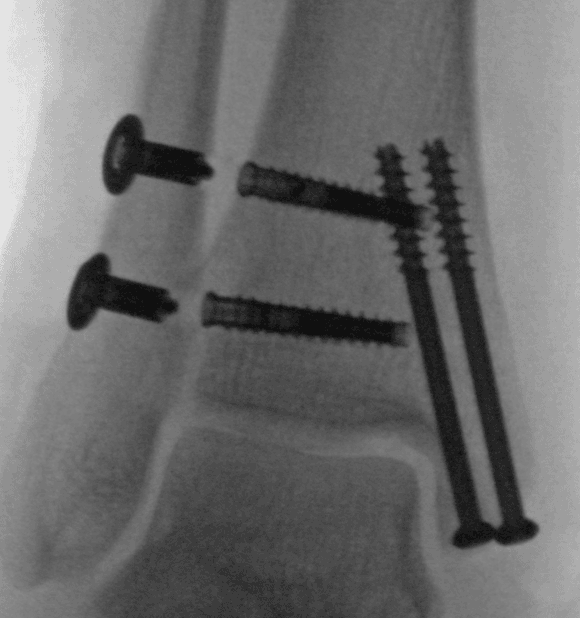
Transverse/oblique medial malleoli fx are commonly fixed using two cannulated screws (shown below) or tension band construct.
Vertical medial malleoli fractures may be repaired with a buttress plate.
Posterior malleoli may be treated with cannulated screw fixation from either A->P or P->A or with buttress plating.
Syndesmotic injury may be treated with syndesmotic screws (shown below) or tight rope.
Complications:
Wound infection
Malunion
Hardware failure
Ankle stiffness
Post-traumatic arthritis
Diabetic patients are at an increased risk of complications. Commonly fixation and time to weight-bearing are enhanced in diabetics.
References:
1: https://www.ncbi.nlm.nih.gov/books/NBK542324/
2: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4075279/
3: https://www.ncbi.nlm.nih.gov/books/NBK542324/